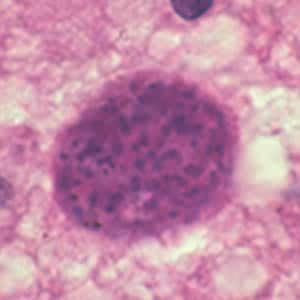
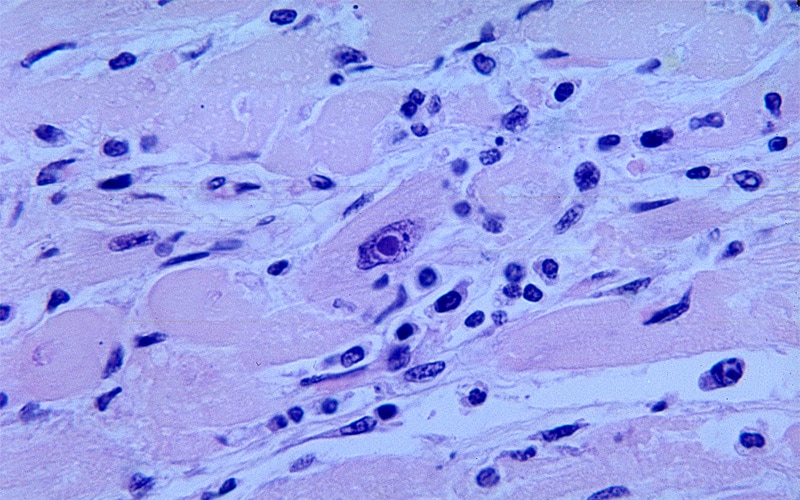
-Cytomegalovirus Infection-

-Cytomegalovirus (CMV) infections are of varying severity and is dependent on the host.
-CMV infections in immunocompetent patients are generally asymptomatic or present as a mononucleosis syndrome
-CMV infections in immunocompetent patients can cause significant morbidity and mortality in organ transplant or organ transplant patients
-CMV is a member of the herpesvirus family
-CMV establishes a latent infection after the resolution of the acute infection
-Productive infection leads to the synthesis of intermediate early, early, and late viral proteins. Viral DNA is detected in monocytes, dendritic cells, and myeloid progenitor cells in the bone marrow
-Secondary, symptomatic disease may present later in life of the host. This comes from reactivation of latent CMV or reinfection with an exogenous novel strain
-High risk for reactivation of CMV may occur in the following conditions: systemic immunosuppression, iatrogenic immunosuppression, and AIDS
-CMV has been cultured from multiple sites including urine, throat, blood, semen, stool, tears and breast milk.
-Transmission of CMV can occur from sexual exposure: contact, blood or tissue, perinatal exposure, and occupational exposure
-CMV can be localized to a single organ or present as a multi-system disorder in a fulminate state
-CMV affects other organs differently
-GI manifestations include colitis, diarrhea, fever, abdominal pain, GI hemorrhage or inflammatory colitis
-Hepatic manifestations of CMV include elevated alkaline phosphatase, and total bilirubin. Portal vein thrombosis can also occur
-CMV can cause neurologic manifestations such as encephalitis, guillian barre syndrome, brachial plexus neuropathy, transverse myelitis, diffuse axonal neuropathy, Horner's syndrome and cranial nerve palsies
-CMV pneumonia can usually only occur in immunocompromised hosts
-CMV retinitis can occur with advance immunosuppression and AIDS
CMV can cause pericarditis, myocarditis, and atherosclerosis
-Enzyme immunoassays and indirect and anti-complement immunofluorescence assays are most commonly used. They measure the presence of anti CMV IgM and IgG
-The detection of CMV specific IgM antibodies are useful in newborns
-Most cases of primary CMV infection in immunocompetent hosts occur and pass with no or minimal symptoms.
-Agents available for systemic treatment are usually used only on immunocompromised patients. Antivirals for CMV include: ganciclovir, valganciclovir, fosacarnet, and ciodfovir
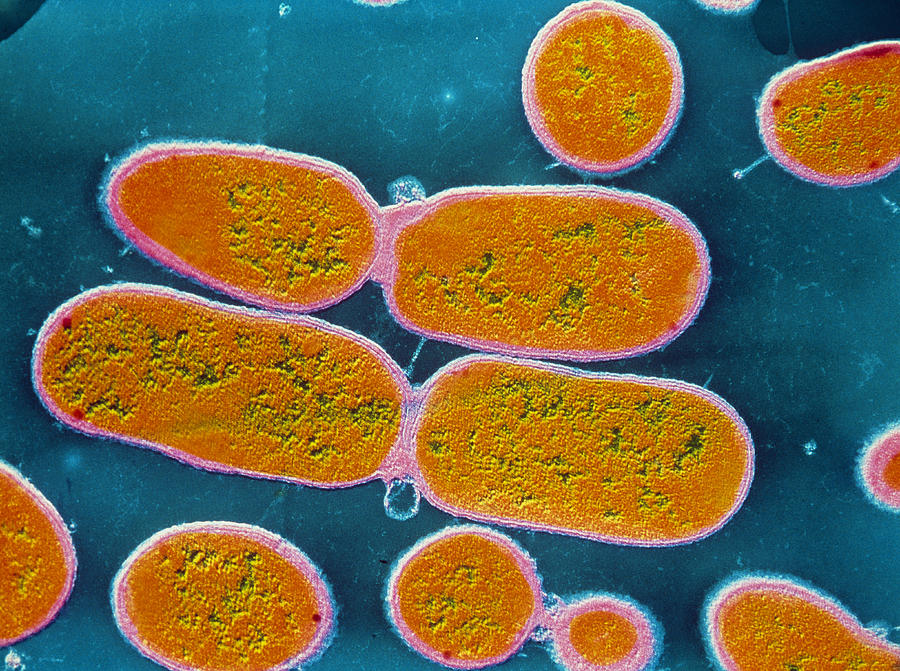
-Epstein Barr Virus-
-Epstein Barr Virus (EBV) is a herpes virus that is spread by contact with susceptible persons and asymptomatic carriers of EBV
-EBV is the infectious agent of infectious mononucleosis
-EBV is associated with the development of B cell lymphomas, T cell lymphomas, Hodgkin lymphoma, and nasopharyngeal carcinomas
-EBV has a latency phase as well as an infectious phase
-Infectious Mononucleosis presents with malaise, headache, low grade fever, sore throat, lymphadenopathy(usually anterior and posterior cervical) and moderate to high fever
-With infectious mononucleosis there is a large percentage of atypical lymphocytes
-Fatigue can be the predominant symptom. Other less common physical exam findings include: palate petechiae, periorbital or palpebral edema, and maculopapular rashes
-Nausea, vomiting, and elevated transaminases are found in a good percentage of patients from associated hepatitis. Splenomegaly is common
-EBV can affect virtually any organ system and can be associated with pneumonia, myocarditis, pancreatitis, mesenteric adenitis, myositis, glomerulonephritis, Guillain Barre syndrome
-There is a specific drug disease specific interaction between mononucleosis and ampicillin
-Oral hair leukoplakia development can happen as a mucocutaneous manifestation of EBV
-Splenic rupture is a rare but fatal complication of infectious mononucleosis. Contact sports athletes need to be kept out of sports until splenomegaly resolves
-Burkitt Lymphoma is the most common childhood malignancy in Africa. It is associated with EBV and is usually localized to the jaw.
-Diagnosis can be confirmed by the monospot test which assesses heterophile antibodies
-IgG antibodies to early antigen are present at the onset of the clinical illness.
-The treatment of mononucleosis is supportive. Analgesics, anti-pyretics, and fluid hydration are supportive measures
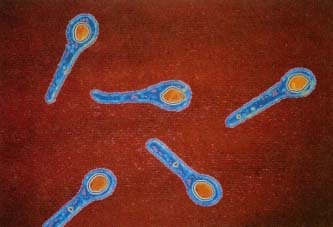
-Erythema Infectiosum-

-caused by the Human Parvovirus B19
-get diffuse erythema rash and edema to the cheeks
-get a "slapped cheek" appearance
-prodrome of fever, malaise, headache, coryza, itching, myalgias and sore throat
-several syndromes associated with parvovirus B19 include: Fifth's Disease, Arthropathy, Transient Aplastic crisis with chronic hemolytic disorders, non immune hydrops fetalis, intrauterine death, and hemolytic disorders
-Parvovirus B19 is also associated with myocarditis, dilated cardiomyopathy and left ventricular dysfunction
-pathogenesis of rash is not clear but correlates to serum antibody levels
-management is symptomatic
-Herpes Simplex-
-Herpes simplex virus has two major types HSV type 1 and type 2
-HSV 1 is also known as herpes labialis often referred to as cold sores
-HSV type 1 can also occur at other locations than the lips. HSV type 1 can be found in the genitalia, liver, eyes, and the central nervous system.
-HSV type 2 is usually specific to genitalia
-When HSV type 1 is in other locations that the lips, it is usually severe infections in the setting of immunosuppression
-HSV type 1 is transmitted at mucosal surfaces or skin sites that permits entry to the epidermis, dermis, and the sensory and autonomic nerve endings
-The cutaneous lesions of HSV present as grouped vesicles on an erythematous base
-When an HSV infection has occurred, the virus lives in the nerve cell bodies in a latent phase until it reactivates
-Precipitating factors for HSV 1 reactivation include: fever, sunburn, trauma, and menstruation
-HSV infection of a finger is known as a herpetic whitlow
-HSV Type 1 is associated with onset of erythema multiforme
-Ocular HSV infections cans cause keratitis and acute retinal necrosis
-HSV type 1 can also cause encephalitis or aseptic meningitis
-Fulminant hepatitis is rare but a complication of an HSV infection. Occurs with immunocompromised patients
-Immunocompromised patients also can get HSV esophagitis and HSV pneumonitis
-Diagnosis can be confirmed by viral culture and Tzanck smear
-Acyclovir, famciclovir, and valacyclovir all interfere with viral replication of the virus. Famciclovir and valacyclovir have higher oral availability.
-Topical anti-viral agents have marginal benefit and should really not be used
-Parenteral therapy should be used for more severe infections such as: CNS infections, transverse myelitis, end organ disease (hepatitis or pneumonia), and disseminated HSV
-Anti-viral therapy is most helpful if initiated in the first 72 hours
-Patients can also be offered daily suppressive therapy who have frequent outbreaks
-HIV Infection-

-Human Immunodeficiency Virus (HIV) infection has several stages:
1. Viral Transmission
2. Primary HIV infection
3. Seroconversion
4. Early symptomatic HIV infection
5. AIDS (CD4 count less than 200/mm3)
6. Advanced AIDS (CD4 count less than 50/mm3)
-Initial testing should include forth generation HIV 1/2 immunoassay, if negative no further testing is required.
If positive should have HIV 1 and 2 antibodies evaluated. If indeterminate, check for RNA to see if acute HIV1 infection or not
-Viral transmission comes from sexual intercourse, exposure to contaminated blood, or perinatal transmission
-Heterosexual transmission is the most common reported mode of viral transmission in women
-Risk factors for HIV transmission include: viral load, lack of circumcision, sexual risk, nitrate inhalant use, and ulcerative genital STD's present at time of intercourse
-Most patients seroconversion occurs to positive HIV serology within 4-10 weeks
-The period of early HIV disease extends from seroconversion to six months following HIV transmission
-During asymptomatic infection, patients may have no findings except possible generalized lymphadenopathy
-Signs and symptoms of acute symptomatic HIV infection include: fever, fatigue, myalgias, adenopathy, oropharyngeal edema, tonsillar enlargement, painful mucocutaneous ulcerations, rashes, nausea, diarrhea, anorexia, headache and retroorbital pain, and dry cough
-Conditions that define AIDS diagnosed P. Carinii, Esophageal Candidiasis, Wasting, Kaposi Sarcoma, HIV associated dementia, CMV, Toxoplasmosis, Immunoblastic lymphoma, chronic cryptosporidiosis, Burkitt Lymphoma, Disseminated Histoplasmosis, Chronic Herpes simplex
-Once the decision is made to treat an acute or early HIV infection, the choice of treatment should be guided by drug resistance testing
-Common antiretrovirals include ritonavir, atazanavir, darunavir with tenofovir emtricitabine
-Once treatment is initiated, it should be continued indefinitely
-Human Papilloma Virus Infections-

-Human Papilloma Virus (HPV) is a DNA virus
-HPV is the most common sexually transmitted infection in the US
-HPV is associated with condyloma acuminata, cervical cancer, vaginal cancer, vulval cancer, anal cancer, squamous intraepithelial lesions and malignancy, and head and neck malignancy
-High Risk HPV Genotypes (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68)
-Low Risk HPV Genotypes (6, 11, 40, 42, 43, 44, 53, 54, 61, 72, 73, and 81)
-Genotypes 16 and 18 of HPV are the most common types found in cervical cancer
-HPV is also implicated in oral cancers and pre-cancer lesions
-Risk factors for HPV infection include unprotected penetrative intercourse or close skin contact of the involved area. Digital/anal and digital/vaginal contact can cause spread of the virus
-Detecting HPV can be done by HPV DNA and RNA testing. Can also detect cellular markers
-Prevention of spread of the virus is the best treatment. Patients that test positive for HPV need closer surveillance (ex pap smears)
-Influenza-

-Influenza is an acute respiratory illness caused by the Influenza A and B viruses
-Transmission of the virus is by respiratory secretions
-Generally speaking, viral shedding can be detected 24-48 hours before the onset of symptoms, but much lower during the symptomatic period of the illness
-Uncomplicated influenza presents with fever, headache, myalgias, nasal congestion, non productive cough, and sore throat. Physical exam is usually unremarkable
-Pneumonia is the most common complication of influenza
-Myositis and rhabdomyolysis are also complications of influenza
-CNS complications of influenza include: encephalopathy, encephalitis, transverse myelitis, aseptic meningitis, and Guillain Bare Syndrome
-Two classes of antiviral drugs available for treatment of influenza-
1. Neuraminidase inhibitors such as zanamivir and oseltamivir are active against influenza A and B
2. The adamantanes such as amantadine and rimantadine that are active against influenza A
-These agents can shorten the duration of the illness 12 hours to 3 days. Most studies have shown benefit when instituted 24-48 hours from the onset of symptoms
-Institution of any antivirals is recommended when: illness requiring hospitalization, age over 65, pregnant women or post partum less than 2 weeks, or progressive, severe or complicated illnesses-High priority age groups for influenza vaccine: pregnancy, immunocompromised patients, healthcare workers and household contacts
-Measles-

-Measles (Rubeola) virus is a member of the Paramyxovirdae family
-highly contagious childhood viral infection
-Stages of infection include: incubation, prodrome and then exanthem
-Individuals are asymptomatic usually during incubation period
-highly contagious childhood viral infection
-Stages of infection include: incubation, prodrome and then exanthem
-Individuals are asymptomatic usually during incubation period
-Prodrome presents with fever, coryza, cough, congestion, conjunctivitis, and Koplik spots
-Koplik spots are 1-3 mm whitish, gray, or blue elevation with an erythematous base, usually seen on buccal mucosa opposite molar teeth
-see in patients that are not immunized
-caused by measles virus and paramyxovirus
-Measles in pregnancy appears to be a risk for serious maternal and fetal complications
-Diagnosis is made by anti-measles IgM which can be detectable 3 days after the appearance of the rash
-Treatment is symptomatic
-Mumps-

-Mumps is a RNA virus that is from the Paramyxovirus family
-Mumps is a self limited viral syndrome
-Mumps has a nonspecific prodrome consists of low grade fever, malaise, headache, myalgias, and anorexia
-The prodrome is proceeded by parotitis which is characteristic of mumps infection
-More serious complications of mumps include meningitis, encephalitis, and orchitis
-Less frequent complications arthritis, pancreatitis, and myocarditis
-Diagnosis is made by positive IgM mumps antibody, significant rise in IgG titers, and isolation of mumps virus in a specimen
-Treatment is symptomatic
-Rabies-
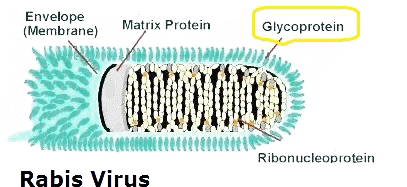
-Rabies has the highest case fatality rate of any infectious disease
-Most rabies is spread by exposure to saliva from the anima bite
-In developed countries, dogs account for spread of 90 percent of rabies cases. This was essentially eliminated as a source in the 1970's
-There are 4 major reservoirs for rabies in US: bats, skunks, raccoons, and foxes
-As a general rule small rodents such s rats., mice, squirrels, gerbils, and chipmunks are susceptible but are uncommon in these animals
-Incubation period on average is 1-3 months, but can range from several days to several years after exposure
-Prodrome symptoms of rabies can include: low grade fever, chills, malaise, weakness, fatigue, anorexia, sore throat, nausea, vomiting, headache, and photophobia
-Clinical rabies may involve two forms of the disease including: encephalitis (furious) or paralytic (dumb) rabies
-Encephalitis rabies is the most common form of rabies
-Encephalitis (Furious) rabies symptoms include hydrophobia, pharyngeal spasms, fever, and hyperactivity leading to paralysis, coma and then death
-Paralytic (Dumb) rabies presents with ascending paralysis and can mimic Guillian Barre Syndrome
-Most patients with rabies die within two weeks after then onset of coma. Most patients die because of asphyxiation and respiratory arrest from muscle spasms or uncontrolled seizures in encephalitic rabies and paralysis from paralytic rabies
-The diagnosis of rabies can be made by skin biopsy before death by virus specific immunofluorescent staining or detection of anti-rabies antibodies in the serum or CSF
-Post mortem testing involves brainstem and neural tissues directly of infecting animal or patient
-In general, rabies cannot be effectively treated so needs to be prevented
-There is no proven antiviral therapy for rabies but Ribavirin and Amantadine have showed in vitro activity. Neither have been studies in clinical trials
-There is no proven role for the rabies vaccine or immune globulin in patients with established rabies
-Rabies immunoglobulin is known as passive immunization and rabies vaccine is active immunization
-Rabies vaccine alone should be given for preexposure prophylaxis
Post-exposure rabies prophylaxis should include the rabies vaccine and immunoglobulin
-Half of the injection in given around the wound and the other half is given intramuscularly as an injection
-Thorough washing of wound and non bite exposures with soap and water is recommended. A virucidal agent such as povidone and iodine should be used
-Roseola-

-Roseola infantum (sixth disease, pseudorubella, and 3 day fever) is a viral clinical syndrome characterized by 3-5 days of high fever that resolves abruptly and is followed by development of a rash
-Roseola usually is caused by human herpesvirus
-The fever or Roseola may have a fever that exceeds 40 degrees C (104 degrees F)
-Clinical manifestations of Roseola include: malaise, palpebral conjunctivitis, edematous eyelids, inflammation of the tympanic membrane, oropharyngeal junctional macules or ulcers, upper and lower respiratory symptoms, vomiting, diarrhea, sterile pyuria, and bulging fontanelle, cervical post auricular occipital lymphadenopathy
-Roseola is usually diagnosed on clinical features and laboratory evaluation is seldom necessary
-Roseola is self limiting and treatment is symptomatic
-Rubella-

-Rubella virus is a member of the Togavirus family. Rubella is a RNA virus
-Rubella has an incubation period of 14-18 days
-Rubella is acquired via inhalation of infectious large particles aerosols and is augmented by close and prolonged contact with infected individuals
-Infected individuals are contagious 1-2 weeks before the infection becomes clinically apparent
-Many infections of rubella are generally mild and many are subclinical or asymptomatic
- Clinical manifestations of post-natal rubella can include maculopapular rash, low grade fever, lymphadenopathy (posterior cervical, posterior auricular, and sub occipital). Arthralgias may persist for up to one month
-Congenital rubella syndrome has defects such as hearing loss, mental retardation, cardiovascular defects, and ocular defects
-Specific IgM antibody can be detected as early as 4 days after the onset of the rash and can be detectable for 6-8 weeks after the infection
-Viral isolation from nasopharyngeal secretions can be used to confirm an acute rubella infection during pregnancy
-Treatment is supportive
-Varicella-Zoster Virus Infections-

-Varicella Zoster Virus (VZV) causes two distinct forms of the disease
-Primary VZV infection causes varicella (chickenpox) characterized by vesicular lesions in different stages of development on the face, trunk, and extremities.
-Herpes zoster (shingles) results in reactivation of the endogenous latent VZV infection within sensory ganglia
-The clinical form of shingles is painful unilateral vesicles erupted in a dermatomal distribution
-The clinical form of herpes zoster is characterized by the rash and neuritis
-Recurrent zoster in an immunocompetent host is uncommon
-Complications of zoster include post herpetic neuralgia, bacterial skin infection, ocular uveitis and keratitis, motor neuropathy, meningitis, and herpes zoster oticus (Ramsay Hunt Syndrome)
-Diagnosis is usually clinical but techniques for lab confirmation include viral culture and direct immunofluorescence testing, and PCR assay
-Treatment for VZV includes symptomatic treatment and antiviral therapy
-Acyclovir is the only antiviral therapy available for primary varicella in both healthy and immunosuppressed patients. There is no clinical data for famciclovir or valacyclovir